May is Melanoma and Skin Cancer Awareness Month. This is appropriate because the weather is getting warmer and more people are spending more time outside in the sun. We want to ensure all of our readers are properly educated on signs, symptoms, risk factors, and treatment options for skin cancer. Skin cancer may be the most common type of cancer, but it also cancer you can SEE and cancer that is very curable if caught EARLY! Now is a great time to get a full-body skin check to find out if you have any suspicious lesions that could be cancerous. Earlier detection of skin cancer means easier treatment and smaller scars.
Skin cancer is the most common type of cancer in the United States followed by breast cancer and lung cancer. There are three main types of Skin Cancer: Basal Cell Carcinoma, Squamous Cell Carcinoma and Melanoma. Early detection of skin cancer is key for the best possible treatment outcomes and cures.
Basal Cell Carcinoma

What does it look like?
Basal cell carcinomas (BCC) are typically pink and pearly and often look like a pimple or a bug bite that will not heal. Sometimes they can even look like a patch of eczema or psoriasis that doesn’t respond to steroid creams. Basal cell carcinomas are commonly found on sun-exposed areas of the skin. They are the mildest form of skin cancer and do not tend to spread to other organs. There are some invasive or more aggressive types of basal cells too, but usually basal cell carcinomas just sit on the surface of the skin and grow there. In general, they are usually easy to treat and cure, especially if they are found early.
How do you treat it?
There are a few different ways you can treat basal cells. Probably the most common way to treat a basal cell carcinoma is a procedure called electrodessication and curettage, or EDC. Some people call it the scrape and burn method. They can also be cut out and closed with stitches. Nova Dermatology offers both of those procedures in the office. Another common procedure is called Mohs surgery. It is a special type of skin cancer surgery reserved for skin cancers on certain areas of the body, like the head and neck or for large or very invasive basal cells. Specially trained dermatologic surgeons perform Mohs.
What are my risk factors?
Risk factors for basal cell carcinomas include:
- Ultraviolet light exposure from the sun or tanning bed use
- Fair skin
- Over the age of 50 years
- History of previous BCC or other types of skin cancer
- Chronic skin inflammation from previous injuries like burns or scars
Squamous Cell Carcinoma

What does it look like?
Squamous cell carcinomas (SCC) tend to be thick, red or yellow, crusty bumps or patches. Sometimes people think it is a wart, skin tag, or crusty scab. These can also look like a rash that will not go away. Sometimes these grow from a precancerous lesion called an actinic keratosis. While squamous cell carcinomas are most commonly found on areas of the body that have had a lot of sun exposure, they can also be found on the genitals, especially if there is a history of genital warts. Like BCCs, squamous cell carcinomas can also be superficial or invasive, but the invasive ones can metastasize or spread to other organs, so those are not considered to be quite as wimpy as basal cells.
How do you treat it?
Like basal cell carcinoma, the very superficial squamous cell carcinoma in situ, or SCCIS, can also be treated with the scrape and burn method. Otherwise, depending on the location, you will probably need an excision or the Mohs procedure.
What are my risk factors?
Risk factors for squamous cell carcinomas include:
- Ultraviolet light exposure from the sun or tanning bed use
- Fair skin
- Over the age of 50 years
- History of previous BCC or other types of skin cancer
- Chronic skin inflammation from previous injuries like burns or scars
- Weakened immune system from medications needed after an organ transplant or for certain illnesses
- History of the Human Papilloma Virus (HPV)
Melanoma
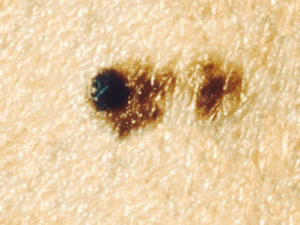
What does it look like?
Melanoma is the most serious type of skin cancer because these spread to other organs of the body the most frequently. These usually look like very dark or black moles that sometimes grow quickly, but occasionally they are pink and look more like BCCs. When evaluating a suspicious mole, we use the ABCDE’s to help us decide if we need to do a biopsy. The alphabet can be very helpful to evaluate suspicious spots that could possibly be melanoma.
Asymmetry– If you draw a line through the middle of a mole, does it look the same on both sides?
Border irregularity– Is the mole perfectly round? Or does it have jagged borders or no borders?
Color variation– Is the mole the same color throughout? Or does it have many colors?
Diameter– Is it larger than a pencil eraser (>6mm)?
Evolution– Is the mole changing in any way?
Some also have added the “EFG rule” to help identify nodular and amelanotic melanomas. Nodular melanomas are usually very symmetrical and do not always have strange colors. They tend to grow very quickly though.
Elevated– Nodular melanomas are elevated, not flat (other types of melanomas can be flat though)
Firm– If you touch the bump, it will feel hard.
Growing– These melanomas grow quickly and need to be addressed quickly too. If you notice a spot that is rapidly growing, it is important to get it evaluated as soon as you can.
The ABCDE’s apply mostly to looking for melanoma, but the “E” applies to any skin cancer. If you notice any spot that has changed or is growing rapidly, or bleeding, then it is a good idea to make an appointment to have it evaluated and biopsied if necessary.
How do you treat it?
We prefer to catch them when they are smaller, but the depth of the lesion is more important than the diameter. So, a special type of biopsy needs to be performed when we suspect melanoma. It is important to get under the entire spot instead of just testing a small piece of these. We usually do what is called an “excisional biopsy” which will require stitches. And, if the results come back positive for melanoma, depending on how deep the mole was according to the dermatopathologist who analyzes it under the microscope, you will either simply need another larger excision or you will need to have lymph nodes removed to see if the cancer has started to spread to other areas. Sometimes additional blood testing or scans such as MRIs, CTs and PET scans are needed.
What are my risk factors?
- Biggest risk factor = Ultraviolet radiation from either the sun or tanning bed use
- Fair skin
- Compromised immune system
- History of other skin cancers or a previous melanoma
- Having many moles; the more moles you have and the bigger your moles are, the greater the chance of developing a melanoma
- Family history and genetics also play a role in your risk for melanoma
What is an Atypical Mole?
Dermatologists will often biopsy a mole because it looks “atypical.” It often has at least one or two of the ABCDEs of Melanoma. There is a spectrum of atypical moles:
Mildly atypical
- Does not need further treatment as these do not seem to have much of an increased risk for turning into melanoma. It is important to keep an eye on the rest of your moles and if new ones pop up or old moles change, we will probably be more likely to biopsy them.
Moderately atypical
- Usually recommended to remove entirely. Also do not have a huge risk of turning into cancer but if the mole grows back partially it will appear misleadingly more suspicious down the road.
Severely atypical
- Must be completely removed as these do have a higher chance of turning into melanoma. May be treated like a melanoma.
Pre-melanoma or Melanoma
- Large excision is warranted to guarantee the entire cancer is removed including any adjacent invasion. Lymph nodes may also need to be removed and tested depending on the depth.
How do I protect myself from the sun?
Proper sun protection techniques are essential as we start thinking about spending more time outside enjoying the warmer weather. There are many ways to protect yourself from the sun’s harmful rays, and it is best to try to do all of them at the same time. The Australians have a catchy way to promote sun protection and help you remember the 5 SunSmart steps
- Slip on clothing- clothes have UPF ratings (see below for an explanation)
- Slop on SPF– use SPF30 or higher broad-spectrum, water-resistant sunscreen.
- Slap on a hat- you need a wide-brimmed hat (not a visor or a baseball hat) so that it helps to cover your ears and back of your neck. If it is a straw hat, make sure it is lined with fabric or a very tight weave, so the sun doesn’t make it through the holes in the hat.
- Seek shade- Try to avoid going out in direct sunlight when the sun’s rays are the strongest. From 9 am until 4 pm you should pay particular attention to protecting yourself. Try to stay covered under the shade using trees or umbrellas or tents when you are out. Be aware of reflective surfaces, such as snow, water, or metal, that could be bouncing the rays back up to you even though you are shaded from above!
- Slide on sunglasses- It is important to protect your eyes from the damaging UV rays too! Look for large, wrap-around and close-fitting sunglasses to reduce reflected UV radiation and glare.
SPF VS. UPF VS. EPF
SPF (Sun Protection Factor)
- A standard measure of the effectiveness of sunscreens. It provides only UVB protection (unless it is labeled as a broad-spectrum sunscreen.) An SPF of 15 prolongs your protection 15 times the time it takes to burn. (So, if your burn time is 15 minutes, then SPF15 should help prolong your time to burn to 225 minutes, or 3 hours and 45 minutes.) You still need to reapply every 90-120 minutes though.
UPF (Ultraviolet Protection Factor)
- Aa standard measure of the effectiveness of sun protective fabrics. It provides both UVA and UVB protection. A UPF of 50 blocks out 49/50 (or 98%) of UV rays when worn. A UPF of 25 means 1/25th (or 4%) of UV radiation can penetrate the fabric. A plain cotton shirt has a UPF of about 5, meaning it only blocks 80% of the radiation. While 80 % block may sound like a good amount, that 20% is still enough for people to get sun burns and skin cancer through a shirt!
EPF (Eye Protection Factor)
Sunglasses have their own UV rating system. The American Academy of Ophthalmology recommends a rating of UV400 or higher. This means it will block up to 99-100% of both UVA and UVB. The Australians, who take skin cancer and sun protection very seriously, have even created their own Eye Protection Factor (EPF) rating. EPF of 9 or 10 is equivalent to UV400 rating. There is also something called the Australian Standard AS1067:2016 for sunglasses, and under that you want to look for lens categories 2, 3, or 4.
When in doubt, get it checked out!
If you have any spots that sound like the above descriptions, or any spots that have changed and look different from how they looked a few months or years ago, then schedule an appointment for a full-body skin check to get those spots and all of your other spots evaluated to see if they need a biopsy.
Skin cancers can recur even after they have been removed properly. It is important to follow up with your dermatology specialist every 6 to 12 months to make sure the site is still healed and also to check for new spots. It is also important to take proper sun avoidance precautions to protect yourself from further sun damage that could cause more skin cancers.
Call Nova Plastic Surgery and Dermatology and book your dermatology appointment in Ashburn, VA now 703-574-2588